EVERYTHING TO KNOW ABOUT BREAST SURGERY
EVERYTHING TO KNOW ABOUT BREAST SURGERY





BREAST AUGMENTATION
WHAT IS THE PERFECT BREAST?
The perfect breast is different things to different people. Our "classy but juicy" version seeks cleavage and lateral fullness that reaches the mid axilla. A sloping breast adds a natural touch. The final result always depends on what you had to start with and the art is in making the most of what you have to work with.
small good breast = bigger good breast
Small perfect breasts result in full perfect breasts unless they are overfilled to distortion. Surgical judgement and esthetic tastes are important at the time of surgery.









THE JUMPING BREAST DEFORMITY

RENOWNED FOR ANALYZING, REPAIRING, AND AVOIDING THE JUMPING BREAST DEFORMITY
DURING THE MORATORIUM ON SILICONE IMPLANTS FROM 1991 T0 2005, DR. VILLAR WAS ONE OF THE RESEARCHERS ALLOWED TO USE SILICONE IMPLANTS IN PATIENTS NOT SUITABLE FOR SALINE IMPLANTS. THIS GAVE HIM THE OPPORTUNITY AND EXPERIENCE TO ANALYZE, REPAIR, AND THEN AVOID THE JUMPING BREAST DEFORMITY. THE SHIFT TO HIGH QUALITY SILICONE IMPLANTS WAS THE TECHNOLOGICAL ADVANCE THAT OFFERED A SOLUTION TO THIS UNATURAL TRADE-OFF IN BREAST AUGMENTATION.
WE CAN FIX IT
BETTER YET, WE CAN AVOID IT.
Augmentations byVillar have optimal cleavage and DO NOT JUMP.
POOR CHOICE EQUALS POOR RESULTS
This patient should not have had implants under the muscle because she had very wide spaced breasts to begin with. Wide jumping breasts. Poor choices lead to poor results. There is a Better Way.
JUMPING BREAST DEFORMITY
The jumping breast deformity results from placing implants UNDER the muscle. The pectorals muscle is divided medially, retracts and attaches to the breast tissue. When contracting , it pulls the breast up and out. It can be a small pull or greatly exaggerated . This deformity can be avoided by placing silicone Implants OVER the muscle. A large part of our practice is correcting this deformity which involves removing the implants, suturing the muscle back to the chest wall, and replacing the implants OVER the muscle in the sub-mammary plane. This also improves the wide cleavage often associated with this.


when to go over the muscle
Patients who have widely spaced breasts should avoid implants UNDER the muscle. In these patients, the medial muscle insertion is widely spaced. When the implant is inserted, it can not go more medially than the insertion, thus the cleavage is wide. The muscle is cut to accommodate the implant. It retracts and attaches to the Breast tissue. When it contracts, it deforms the breast laterally. (jumping breast deformity) These patients have better cleavage and no jumping deformity with the implant OVER the muscle, under the breast tissue.
Patients with tight cleavage and abundant breast tissue can tolerate sub pectoral implants. Skilled surgeons fit the surgery to the patient. Assembly line surgeons fit patients to their one surgery.
The main argument is that over the muscle implants have a greater chance of capsular contracture. For arguments sake, let’s say under the muscle is 1% contracture and over is 2% contracture. The way I look at it, to save one patient in ten from contracture, you are creating nine, ugly wide cleavage jumping breasts. I prefer to get eight beautiful breasts sacrificing the one extra to capsular contracture. Now, there are patients that have tight cleavage and enough breast tissue to hide under the muscle implants and I have no issue with that option. But there are many patients that clearly will get poor results under the muscle. The best surgeons know “one operation does not fit all”.
Check out our work
Best cleavage possible for different types of anatomy and no jumping breast deformity.





























THE INVERTED-T MASTOPEXY - STILL THE MOST RELIABLE TECHNIQUE
Mastopexy is a shrinking operation and augmentation is a stretching operation. They are enemies of each other. I prefer to two stage most of my mastopexies (lift first, then implant later) for safety. But when removing an implant, It is especially important.
With an implant under the breast, there is no central blood supply. The nipple areola is nourished peripherally. If you are planning a long distance move of the nipple nourished on a pedicle, you are a better man than I. You are cutting right into the blood supply.
Then after lifting and tightening up the breast (shrinking procedure), if you stuff an implant into the pocket (stretching procedure) you dramatically decrease your margin of safety. Any post operative swelling or hematoma further compromises the blood supply, and by morning a nipple may be irretrievably lost.
I have treated many of these patients treated by competent surgeons willing to take the risk. I have not lost a nipple in my career, either due to my two stage abundance of caution, or I am extremely lucky. And it is true that my mother or someone said “it is better to be lucky than to be good”.
PREOPERATIVE MARKINGS ARE CRITICAL


PREOPERATIVE MARKINGS ARE CRITICAL



FREE NIPPLE GRAFTING
Free nipple grafting is when the nipple areola is removed as a full thickness skin graft using a #15 blade and the new recipient site is de-epithelialized preserving the dermis for its rich blood supply. If you go down to fat, you increase the chance of graft failure. This technique taught to me by Bertram Bromberg is literally a work of artistry and precision.








BAD BOOBS #1. CASE OF THE POLE DANCER
Bunny the pole dancer came to see me for a breast augmentation. I told her that because she had wide cleavage and pole dancing exerts massive pressure on sub muscular implants, she needed silicone implants over the muscle. She could not afford silicone so she went to someone who placed saline implants under the muscle. She returned disappointed with widely spaced door knob breasts. I advised remove and replace implants with silicone over the muscle. She needed 3 months to save money and resumed pole dancing.


detailed video for young surgeons
I produced this video decades ago when I was faced with this challenge. Internal and external sutures common at the time seemed doomed to failure. A novel approach seemed necessary to avoid recurrence
THE IMBRICATION TECHNIQUE

UNIBOOB - SYNMASTIA
Synmastia or UNIBOOB is usually caused by a surgeon trying to improve the cleavage by undermining the medial pectoralis. If the muscle has a large gap between the two sides because of anatomically wide cleavage, the muscle can be totally disconnected allowing the implant and it’s resultant capsule to go across the midline into the opposite breast’s territory.




JILLIANS JOURNEY
AFTER TWO BOTCHED SURGERIES, JILLIAN WAS TOLD FORGET ABOUT IT, THERE IS NO HOPE
Jillian went to her first surgeon without getting a second opinion. He put saline implants under the muscle with a wide cleavage and jumping breast deformity. She then interviewed five surgeons and picked who she thought was best. He worsened her condition. He told her “live with it. What did you want to be, a Playboy Bunny?” For years she thought she was being punished for being vane.




REPAIRING INVERTED NIPPLES
WITHOUT PUTTING UNNECESSARY SCARS ON THE AREOLA
Retracted nipples in youth or after breast feeding are usually benign. However, retraction of a nipple de- novo can result from intra-ductal carcinoma and should be evaluated with a high index of suspicion. The benign form is caused by shortening of the milk ducts.
The ducts are cut through a small incision and the nipple is pulled out. The interior dead space is closed with an absorbable suture, and a purse string nylon suture is run circumferentially on the outside. This is removed at 10 to 14 days. The repair is protected with a corn dressing for three weeks.
BOTCHED BREASTS

30 YEARS OF SECRETLY FIXING THE VICTIMS OF BOTCHED SURGERY
Fixing botched surgery is very risky. If you are not successful, the patient takes their anger out on you, instead of the guy who originally botched the surgery. Dr. Villar had been secretly fixing botched surgeries from around the country to help patients nobody else would help. He was approached by TRUE HOLLYWOOD STORIES INVESTIGATES on the E channel on behalf of one of his patients. The show Plastic Surgery Nightmares, catapulted him to international recognition and served as an inspiration for the series Botched.

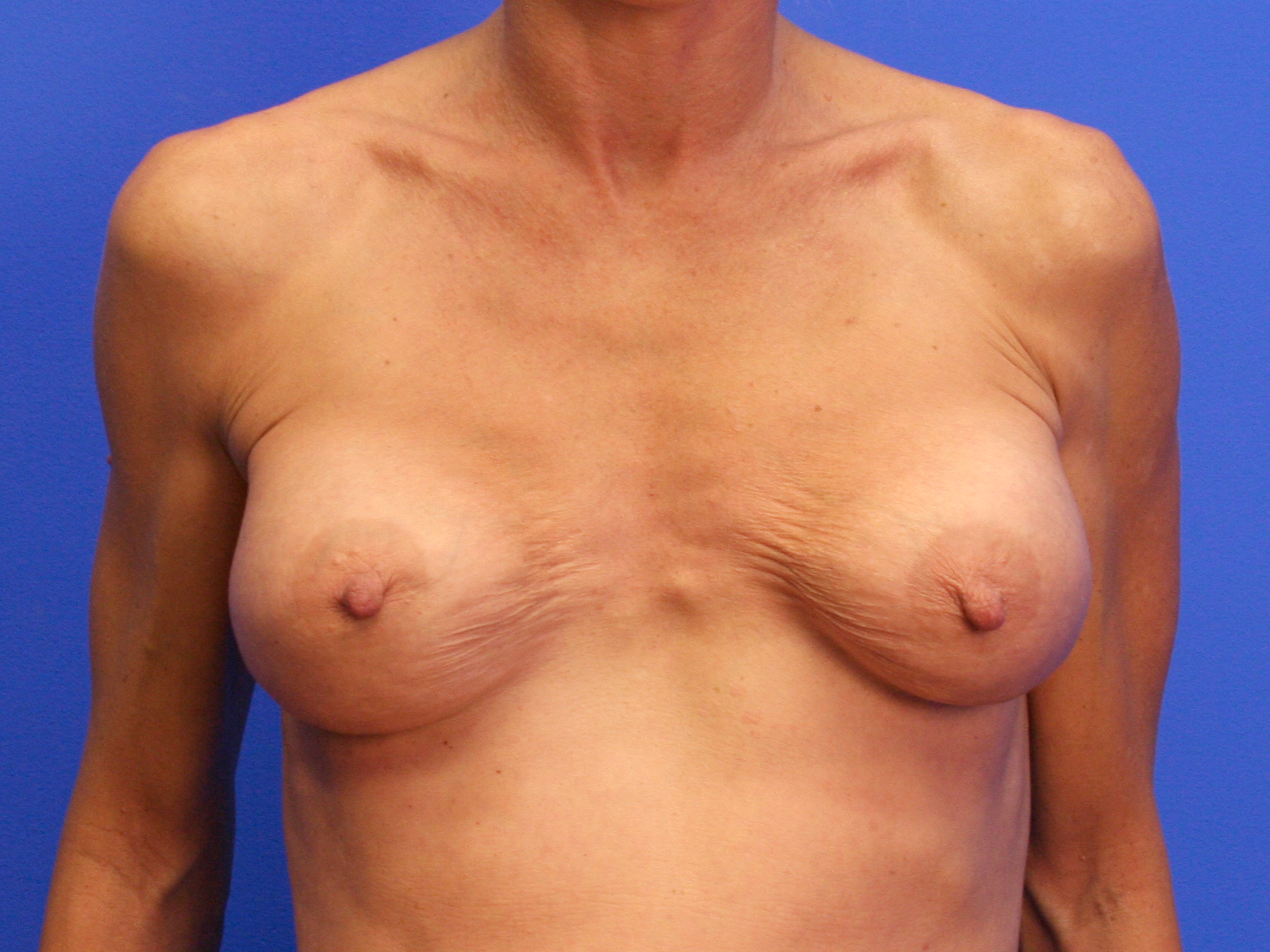
NIPPLE TOO HIGH worst case scenario - FIXING BOTCHED MASTOPEXY
It would be ill advised to lower the right nipple areolar complex in this right nipple too high mistake. It would leave an unsightly scar peeking above a low neckline dress. Instead we will bring the center mass of the breast up under the nipple to point it forward. A prudent compromise for a cardinal blunder.
We will relocate the implant above the muscle to eliminate the jumping deformity.