FACIAL SURGERY
LETS FACE IT....."THERE IS A BETTER WAY"
The master surgeons who took me under wing had a facial surgery common secret. At Massachusettes General Hospital, James May Jr. , one of the greats on the Harvard Surgical Service put his arm around me and whispered.
” When convinced you have mastered a technique to perfection, remember “there is always a better way”.






FACELIFTS
WHAT TO LOOK FOR IN A NATURAL FACELIFT
We have all seen bad facial surgery. The corner of the mouth stretched toward the ears. Corner of the eyes distorted upward. Bloated cheeks from fat injections. Bloated lips that don’t move when speaking. The objective of a natural facelift is to restore the angle of the neck and remove the jowls to restore the jawline and restore cheek fullness. Incisions that allow a pony tail are important.
“There is always a better way”
CHOOSING THE OPTIMAL INCISION for facelift
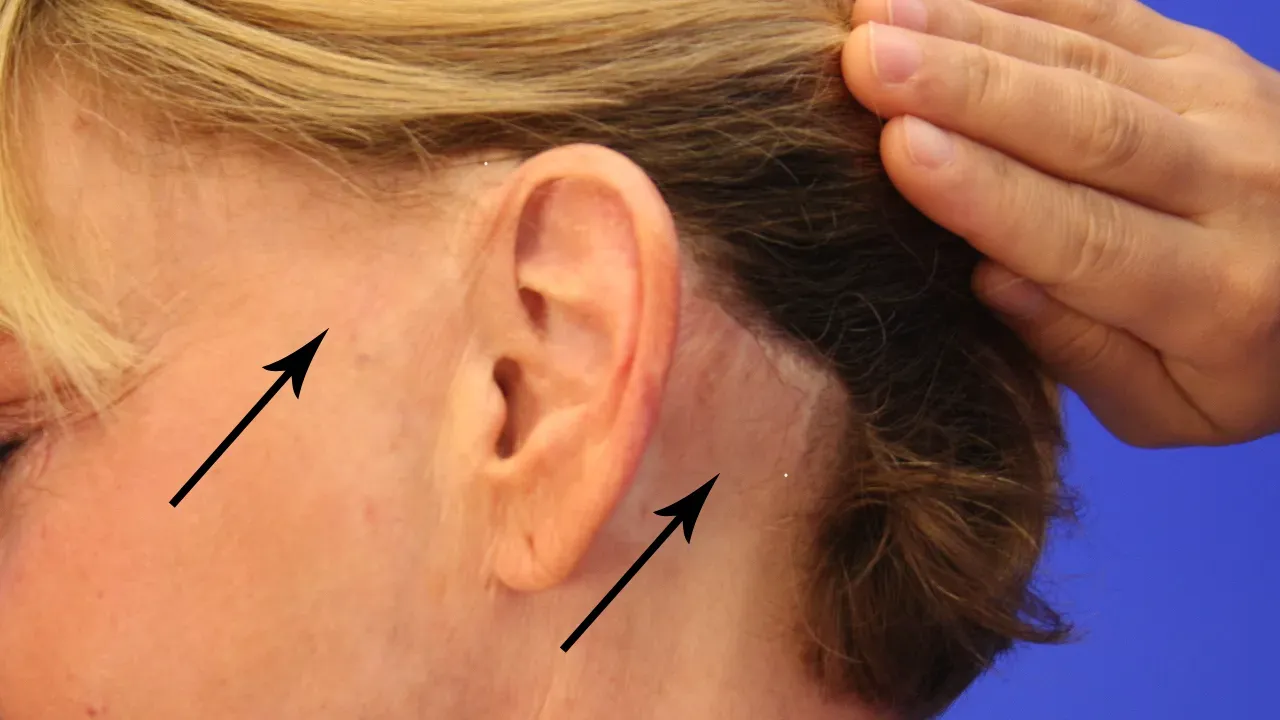
The first sign of a poorly executed face-lift is loss of hair in the temple area and/or behind the ear. This resulted from poor choice of incisions.
CASE STUDIES
DELICATE SHARP DISSECTION RESULTS IN LESS SWELLING, FASTER RECOVERY
Lipodissection, shearing dissection, rough tissue handling and fat injections result in prolonged post op swelling. Delicate sharp dissection along tissue planes and fat injections only when necessary, results in faster facial surgery recovery.

difficult no neck angle case with submental fat and jowls obscuring jawline
This patient was challenging because she had no neck angle and thick sub-mental fat. She fortunately did not have protruding salivary glands. She underwent facelift with platysmaplasty and SMAS plication, The fat was sculptured by sharp dissection rather than lipo-dissection which increases swelling and has a higher incidence of dents in skin. By ten days this difficult case has all sutures out.



difficult no neck angle case with submental fat and long extended jowls obscuring jawline
This patient was challenging because she had no neck angle and thick sub-mental fat. She did not have protruding salivary glands. She underwent facelift with platysmaplasty and SMAS plication, The fat was sculptured by sharp dissection to desired thickness and the excess left on platysma fascia. It is then sucked off muscle with large flat cannula facing down only, to avoid sucking fat off the skin. This results in less denting irregularities, less tissue trauma, and faster recuperation



no neck angle case with minimal sub-mental fat, excess skin and jowls, no protruding salivary glands
This patient was challenging because she had no neck angle excessive skin. She did not have protruding salivary glands. She underwent facial surgery with platysmaplasty and SMAS plication, The excess skin is pulled back with tension behind the ears and trimmed, but in front of the ears the skin is trimmed with no tension to minimize spreading of the scars.




PHENOL PEEL
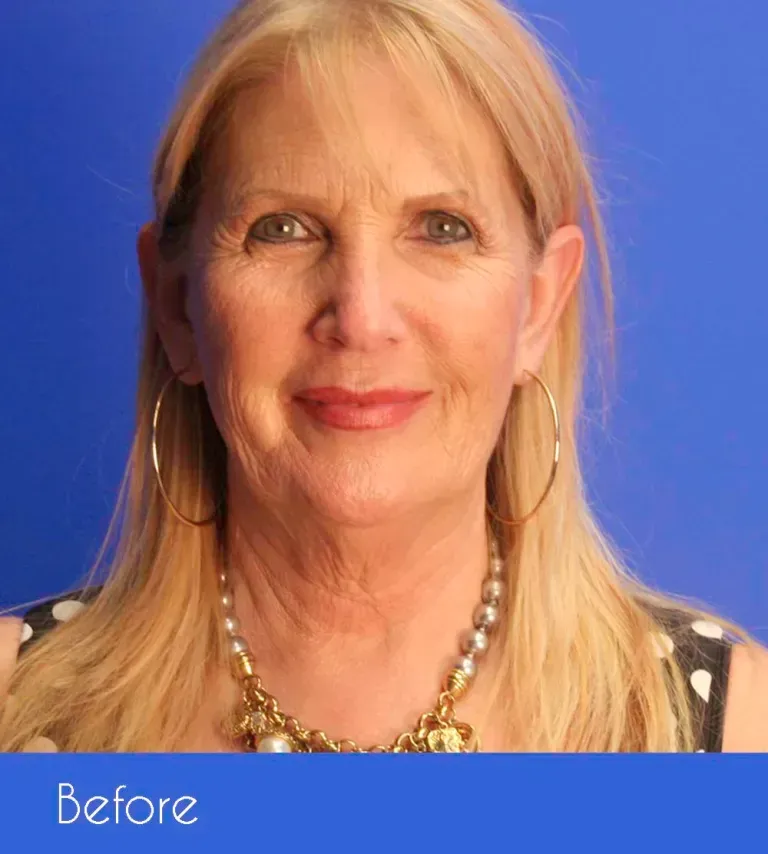
PHENOL PEEL HAS NO EQUAL FOR DEEP ETCHED WRINKLES
Baker and Gordon popularized the PHENOL PEEL decades ago in Miami. It is a mixture of phenol, croton oil, water, and liquid soap. It has to be constantly stirred during application under anesthesia. The patient is kept sleeping for 30 minutes allowing the acid to burn down to the nerve endings to minimize post operative discomfort. Patients will scare animals and small children for exactly two weeks, at which time they can apply makeup and go back to work. They will tighten for up to six months. NO LASER CAN EVER MATCH THE RESULTS! We tried the Coherent CO2 Laser 237 times. Disappointed, we returned back to phenol.

NOTHING ON THE PLANET IS AS EFFECTIVE FOR THESE WRINKLES AS THE PHENOL PEEL
Laser resurfacing was a terrible disappointment. Down time of two weeks was identical, but the laser lasted a year or two compared to a decade with phenol.In our extensive research.




LASER FAILED THE TEST OF TIME
We researched the first Coherent CO2 laser on the Treasure Coast in an attempt to reproduce the amazing effects of the Phenol Peel. The theory was that it is the second degree burn that contracts during the wound healing phase that causes the dramatic results. If we could reproduce the same level of tissue injury, then we should get the same results. This would require a burn that would take exactly two weeks to heal.
For safety, we started with one pass. No good. Then two passes. No good. Then three passes. Some improvement. We eventually perfected the technique with 3 to 5 passes depending on the areas of the face and obtained healing at exactly two weeks without a single injury or scar. Some more enthusiastic practitioners kept going until the wrinkles disappeared and produced third degree burns with catastrophic irreparable scars, especially around the lips!
I was shocked to see on national television a surgeon demonstrating the Coherent CO2 laser with the patient’s face wrapped in tin Foil! What monumental ignorance, I thought!
This laser has a collimated beam. That means the light waves are nearly parallel. They do not focus on a point like some lasers. This is important because a collimated laser beam can go across the room and bounce off reflective surfaces, blinding someone or sparking fire.
After perfecting our technique, we produced a training video which demonstrated the danger of tin foil and the proper us of a wet towel.

AFTER EXTENSIVE EXPERIENCE AND DEVELOPING A RELIABLE AND REPRODUCEABLE TECHNIQUE WITHOUT INJURING ANYBODY, IT BECAME EVIDENT AFTER A FEW YEARS THAT THE LASER RESULTS WERE NOT AS EFFECTIVE AND LONG LASTING AS THE PHENOL PEEL.
WE HAVE ABANDONED LASER RESURFACING AND RETURNED TO PHENOL.
EYELIDS - BLEPHAROPLASTY
WHAT TO LOOK FOR IN BAD EYELID SURGERY
We have all seen bad eyelid surgery. Just look around your favorite restaurant. Do you see the lady or gentleman with the corner of his/her lower eyelid pulled down exposing the white of the eye below the pupil and an almond shaped eye? This is from the novice trying to remove too much skin thinking he can suture it up tight to eliminate the wrinkles. Big and common mistake. The lid will pull down.
There was a school of thought advocating disconnecting the lateral canthus and relocating it higher by drilling a hole in the orbital rim to secure it. This had two complications. We saw the corner of the eye pulled up in an oriental distortion, and if the canthus was stretched too much, the eyelids pinched narrowly. This was likely suffered by Kenny Rogers, the singer.



TRANSCONJUNCTIVAL BLEPHAROPLASTY
In younger patients without excessive skin, the herniated fat bags can be removed from behind the eyelid without leaving a visible scar. This patient in her late 40’s had beautiful skin but the bags made her look very tired in overhead light. The dark lines are not pigmentation but rather shadows cast by overhead light common in the workplace. Slide mouse over photo for before and after. A Video of the procedure is below.
In younger patients with herniated fat but minimal excess skin, the fat can be removed through an incision behind the eyelid. No sutures are required.


CONVENTIONAL BLEPHAROPLASTY
The upper lids have two medial fat pads and excess thin skin causing double folds. The objective is to get a single fold and eliminate the medial fat protrusion. Lower lids have three fat pads. The objective is to remove the fat back to the level of the orbital rim. The common mistake here is to remove too much skin which results in the lid pulling down and exposing white under the pupil. A sight commonly seen in any busy restaurant.








Conventional blepharoplasty is best done under IV sedation so that the patient is not restless and jumping around at the wrong time. The most painful part is removal of the herniated fat which is critical for good results. In a poorly executed upper lid blepharoplasty, you will often notice a bulge of fat just above the medial canthus. Now that the excess skin has been removed, it sticks out like a sore thumb, literally. There are two fat pads here, one yellow, one white and they must be removed back to the level of the orbital rim. Injecting local here distorts the tissue making precision excision more difficult and generating a hematoma in the orbit is the likely source of compression on the optic nerve which has resulted in blindness, a very very very rare occurrence, but none the less a risk.
Patients on anticoagulation should avoid blepharoplasty. Intra or post-op bleeding and hematoma is the most common source of chronic swelling, ectropion, or lid lag. (bad stuff)
Going off anticoagulation for conditions such as atrial fibrillation, has resulted in strokes that have been referred to me for facelifts and eyelid surgeries gone bad.
The story has always been the same. The patient insists that they will take the risk because the surgery is so important to them. The surgeon agrees after the patient signs informed consents.
I learned a valuable lesson after reviewing such a case. The surgeons covered their butt and I held them harmless.
But in my practice, I do not cover my ass. I cover the patient's ass by refusing to do the surgery. I know better and have a duty.
NOSE - RHINOPLASTY



THE MOST CHALLENGING PROCEDURE IN PLASTIC SURGERY
It involves the shaping and relocation of bone, cartilage, and skin, blindly ( by feel ) through two tiny nostrils. In complicated tip cases the columella is transected and the skin peeled up exposing the skin but we try to minimize the open approach because of the unpredictable scar. The bone stays where you put it, and the skin can be manipulated with collgen enzymes, but the cartilage has memory. It has a mind of its own and can twist and turn weeks or months after surgery. This operation is an endeavor of touch and feel engineered in the mind’s eye. It requires great skill and experience plus a good dose of luck. The skill of the surgeon is exposed for all the world to see, when that cast is removed at one week. It is truly one of the most satisfying challenges when all goes well, but just when you think you are the master, Mother Nature will slap you in the face by restoring memory to the cartilage.
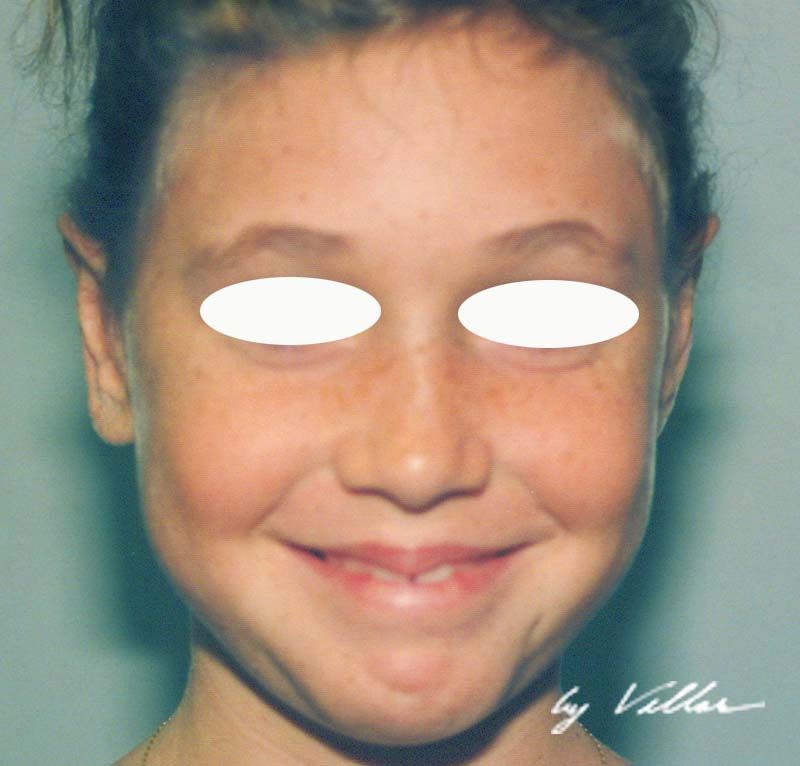
THE RIGHT AND LEFT SIDE OF THE BODY IS ASYMMETRIC BEFORE THE SURGERY
It is important to point out to patients that the right and left side of the body is asymmetric before the surgery. The fetus forms in two neural tubes, like side by side hot dogs. Careful examination will reveal that everything is a little off. Here the left eye socket is lower than the right. The ear lobes are different. The nostrils, corners of the mouth, hands, feet, etc., are asymmetric. The airplane view of the patient is very pleasing, but the fetal development imperfections are present in everyone to varying degrees. Most patients will accept these as a fact of life and derive enhanced self esteem, but a few will dwell on these imperfections and be miserable no matter how nice the nose. It is wise to weed these patients out before surgery and send them elsewhere.



In the 70’s the trend was the turned up nose. The dorsom was lowered dramatically and the distal septum was resected to increase the naso-labial angle dramatically. I never liked looking down someone’s nostrils when talking to them. I was in a movie sitting next to someone with this turned up nose, and when they inhaled the nose would pinch closed with an annoying sound on every breath..
We now understand that removing too much upper lateral cartilage creates a valve effect which closes down the nose with the negative pressure of inspiration. It is important to preserve the form and function of the upper lateral cartilage. My professors performed these turned up noses frequently. They also performed rhinoplasties under local with sedation. Often the patients would wake up choking on the blood and move suddenly compromising a delicate procedure.
When I became Chief Resident, I did all my rhinoplasties intubated under general anesthesia to prevent patients waking up and choking on their blood. I preferred a straight dorsum and did not turn up the tip by resecting the distal septum. These noses appeared more natural to me, and without a pre-operative photograph, it was not obvious they had surgery.
The most difficult cases were the post traumatic badly twisted noses, because cartilage memory is unpredictable.
OTOPLASTY

OTOPLASTY........... RECONSTRUCTION OF THE CUPPED EAR
Otoplasty is the correction of ear deformities which can run the gamut from absence of the ear to the most common which is cupped ear deformity. There are also fistulas, which are vestigial canals when the fat gills incompletely develop into fully formed ears. The fistulas can get chronically infected.
The optimal time for otoplasty is when the ears are fully formed, typically 5 to 7 years old. I prefer to wait until 7 to be sure, but if a child is being teased at school, I will intervene around 5 years old. It is important to understand that not all children that are teased are negatively affected and delaying is to their benefit. Being old enough and healthy enough to tolerate anesthesia in an outpatient facility, usually determined by weight, is a safety factor. If a baby is born with cupped ears, pinning them down with a headband or dressing may correct the deformity before it becomes permanent.
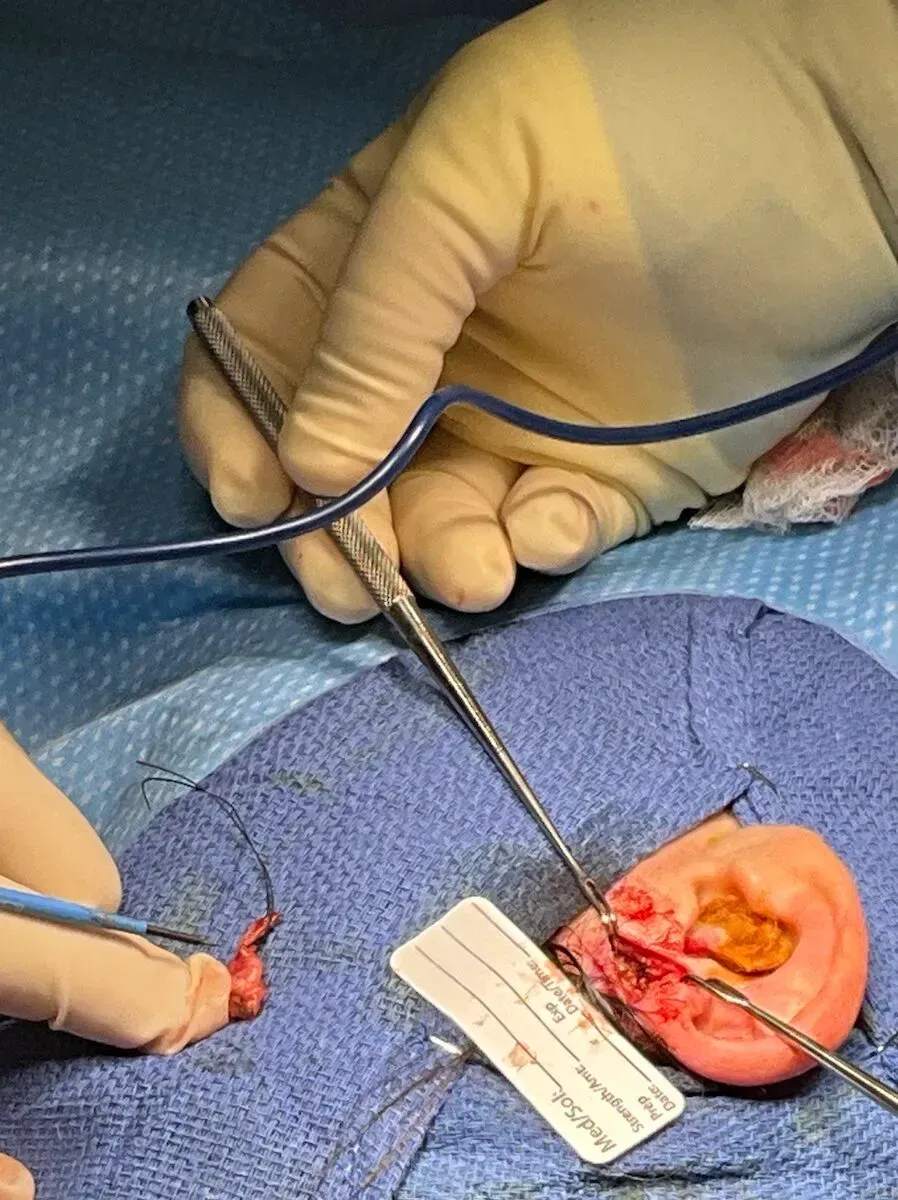
CONGENITAL FISTULAS OF THE EAR
An attempt to simply drain an infection of the fistula was doomed to failure. The canal must be removed back to its source. Here we dissected around the infection and the followed the epithelial lined tube back around the conchal cartilage back to the ear canal shaving off adjacent perichondrium with it.


Morpheus 8

FACE AND NECK SKIN TIGHTENING
SUBMENTAL (UNDER CHIN) SKIN FAT
LARGE PORES, SCARS
CREASES ON THE DÉCOLLETAGE



DON'TS AND DON'TS
THREAD-LIFTS WERE A DISAPPOINTING FAILURE
When the first commercially available thread-lift sutures came out, I was very excited. The initial engineering challenge was how to secure it up in the hairline to sustain the lift long term.
The thread itself was a heavy monofilament that had razor back cuts at an angle. You could pull the suture through tissue in one direction, but when you pulled it back, the back cuts would pop out like little anchors.
The commercial version was a long monofilament with no cutbacks in the middle, then cutbacks on either end terminating in two long needles.
The idea was to make an incision behind the hairline, dissect the forehead off the periosteum, and pass the needle down and out below the eyebrows creating a triangle. The brow would be pushed up with some over-correction, and the hooks would open and anchor the tissue. The filament and needles were snipped at skin level allowing the thread to retract under the skin. I learned leave a little protruding, then cut them at three days so I could still adjust them at the first dressing change.
The learning curve for placement to create the proper arch and how many threads to use, and how much overcorrection was fun. But the big obstacle was how to secure the thread at the apex. Over time sutures under tension cut through tissue and migrate.
So we tried titanium screws, and hand drilling holes in the outer boney plate of the skull.
By the time we solved the fixation problem, the too frequent complications started to show up. The hooks started popping up through the skin, some exquisitely tender, others not. If they broke through pustules would form and the threads had tube pulled out. If a firm downward force was accidentally applied to the brow, the hooks would break loose. I performed a facelift on a volunteer, and long term the threads became palpable, some breaking loose, and hooks protruded.
The complications were so frequent, that the threads were recalled. I had perfected the technique to fifteen minutes for both sides and was terribly disappointed in the long term failures. I cannot recommend thread-lifts.




NEVER HAVE A PEEL AT THE SAME TIME AS A FACELIFT
These permanent scars resulted from an acid peel at the same time as a mid-facelift. Peels over dissected skin are begging for necrosis and scars. Avoidable tragedy. You may get away with it most of the time, but that one patient is ruined for life! Needlessly.